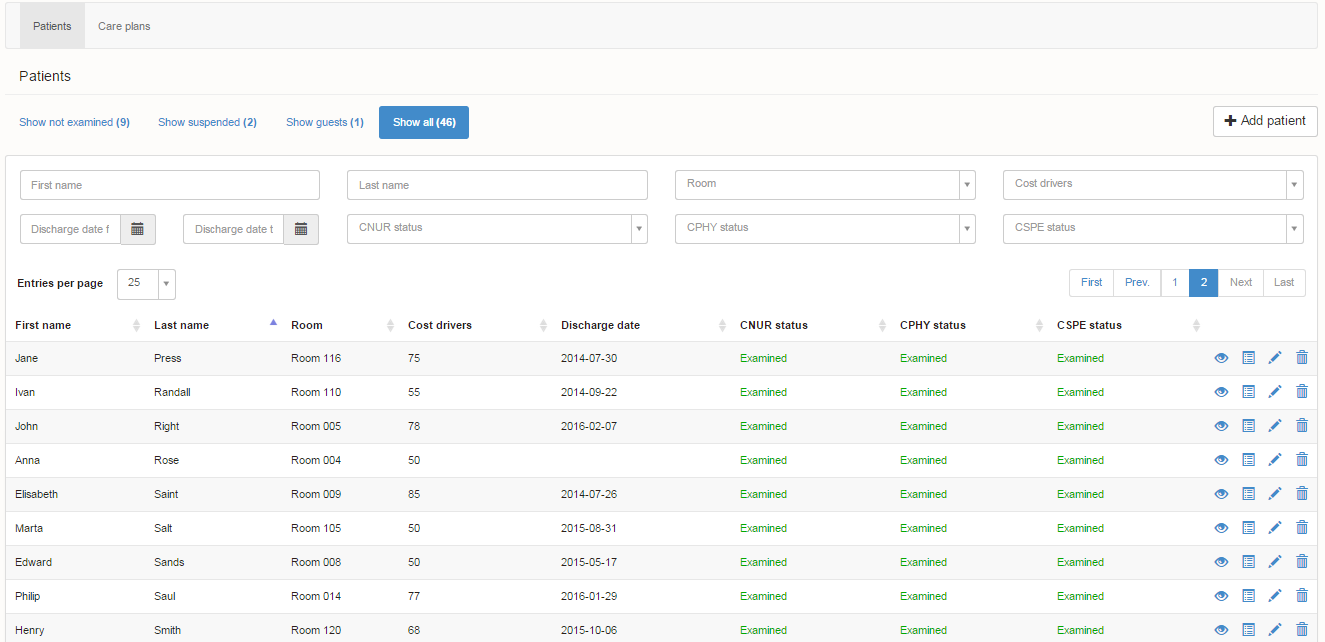
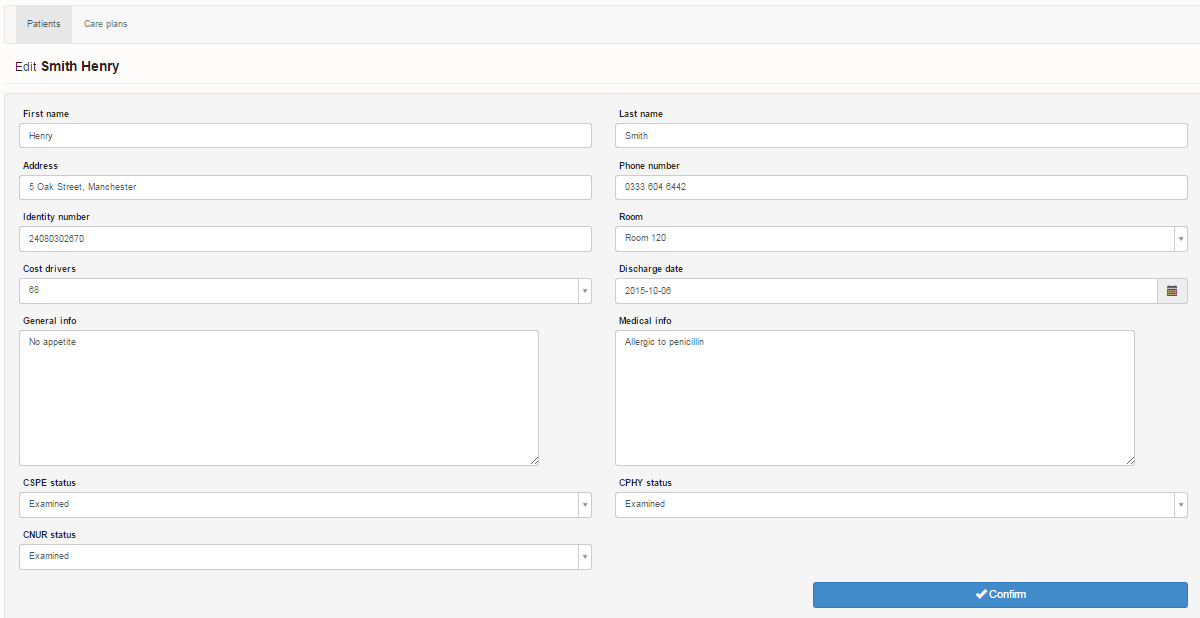
The patient or client record module includes the following:
- Personal data,
- Medical information or assessed care and support needs,
- Patient or client individual preferences,
- Status of the preliminary examination (if applicable).
Preliminary examination may include various areas, depending on the specialisation of the facility, for example: nursing, rehabilitation or mental health. These defined areas are flexible and determined by the organisation.
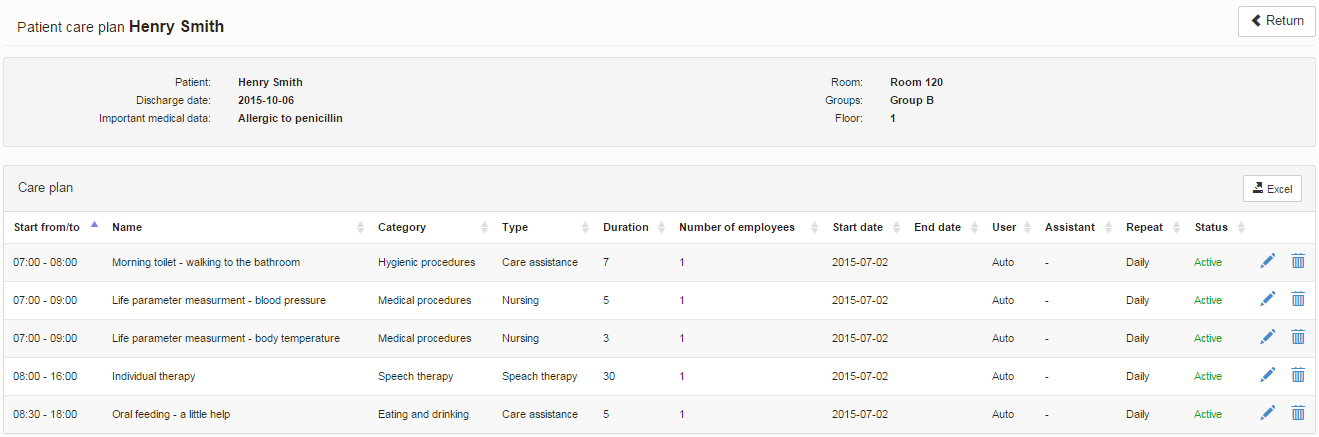
The Individual Care Plan (ICP) is a list of well-defined tasks planned for each patient or client. The ICP is based on the first assessment with the patient or client and their family, medical assessments, care and rehabilitation plan, as well as patient or client preferences, therapeutic and social needs.
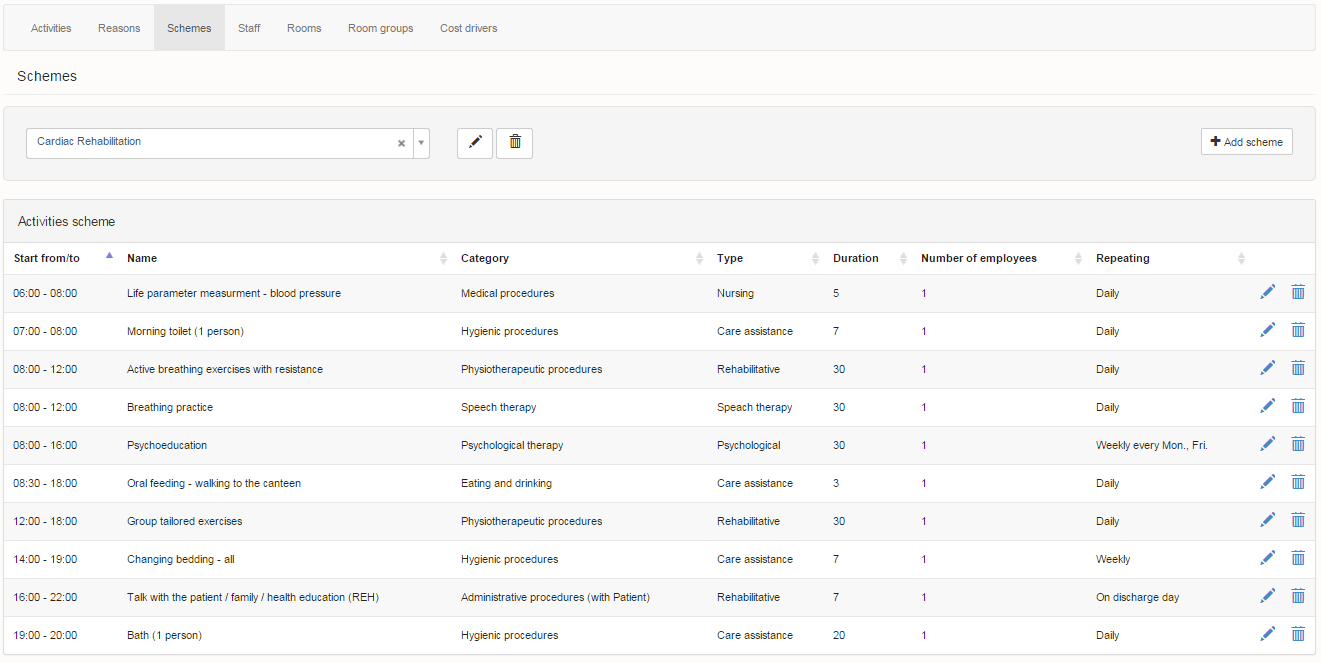
The tasks which form the ICP can be added one by one from the list of more than 300 tasks already defined in the system. Alternatively, there are Care Schemes available in the system that can be selected and later adjusted to meet individual needs and preferences.
Each task has defined parameters such as: optimal duration, priority, starting time, required frequency and staff competency. The parameters of all the tasks are based on practical experience from organisations already using the system. The list of tasks and their parameters are fully customisable.
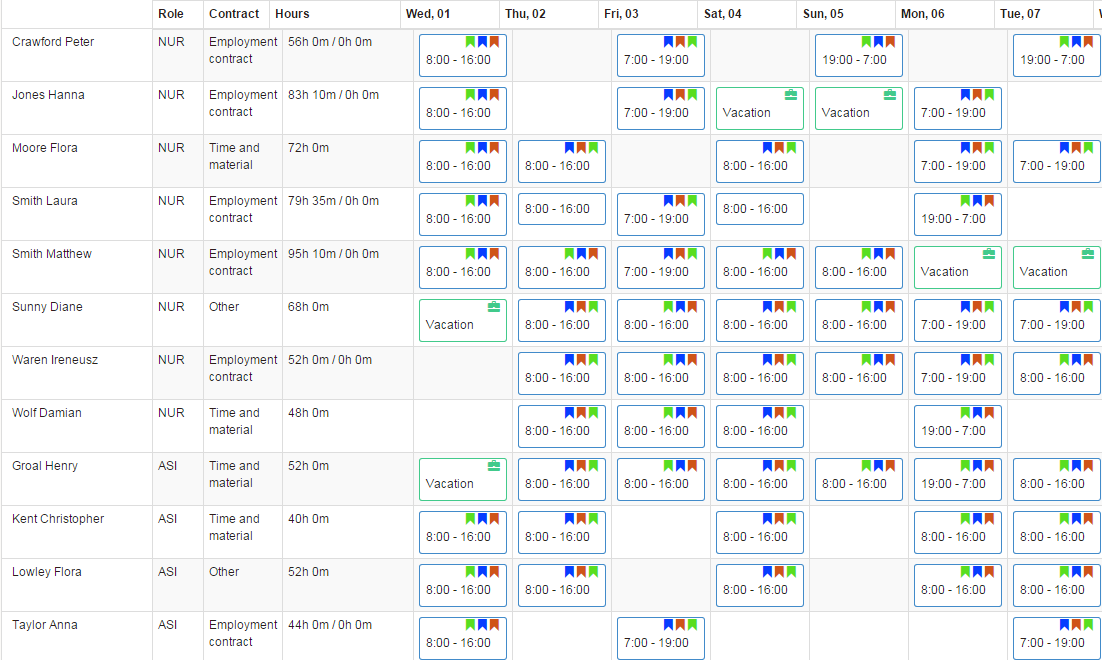
The Rosters module is designed to organise employees’ duty hours. In addition, the system can determine whether the employee will perform tasks across the facility or on certain floors or wards/units. The system facilitates the duties’ planning process by providing information about the number of employees with different competencies that are on duty during that day or night.
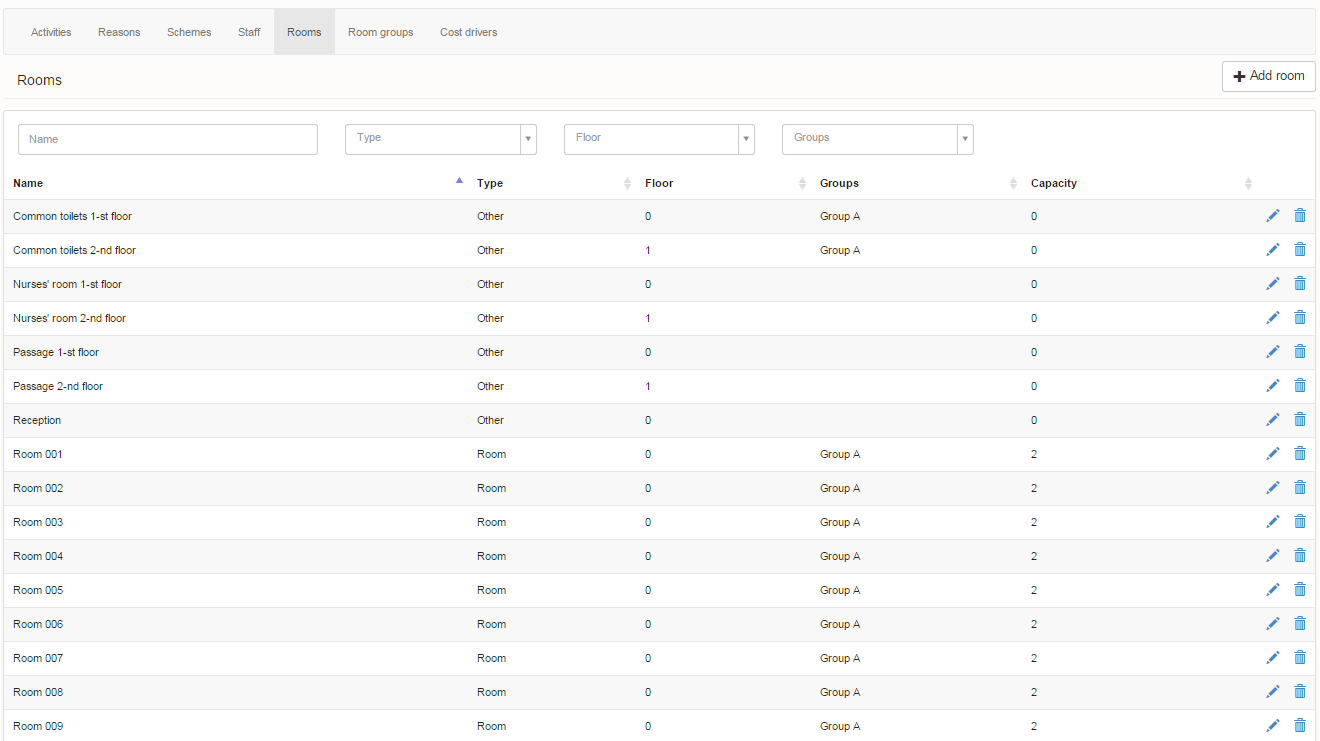

With the Dictionary module, the system can map all the processes that are occurring in the organisation. It includes information related to the infrastructure of the organisation (rooms and floors configuration), calendar (planned holidays) as well as the staff competency (roles and responsibilities). During the implementation phase of the system, after analysing the business processes of the organisation, we define the required information so that work management will be efficient and the work schedule will be optimal.
For example, with the information from this section [infrastructure – visible on screenshots], the system knows how to group activities in different parts of the facility to minimise the distance covered by the personnel while performing their tasks, or how to assign tasks to employees to minimise labour costs.
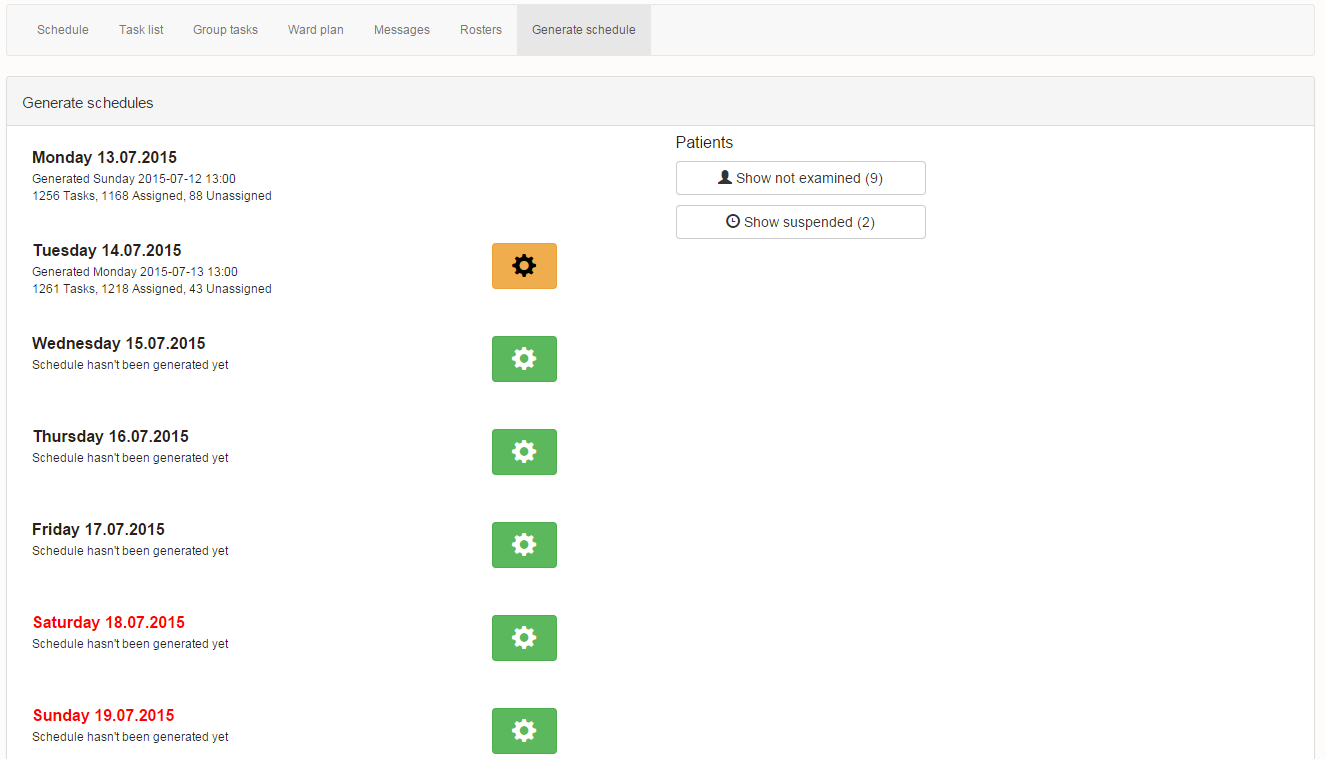
The work schedule is created as a result of the automatic planning. The system collects all the tasks from the ICPs and assigns staff to perform them by taking into account all the parameters of the activities (duration, priority, linkages etc.), staff (availability, competencies, roles etc.) and patient or client (availability, preferences etc.), and at the same time following more than 50 optimisation rules. The generated tasks are presented graphically in the Schedule module.
The Schedule module allows the Care Manager to monitor and control the execution of tasks. The system also notifies them about unperformed tasks, enabling them to rapidly diagnose the situation and respond to it.
The work schedule is created as a result of the automatic planning. The system collects all the activities from the Individual Care Plans and assigns staff to perform them by taking into account all the parameters of the activities (duration, priority, linkages etc.), staff (availability, competencies, roles etc.) and patient/client (availability, preferences etc.), and at the same time following more than 50 optimisation rules.
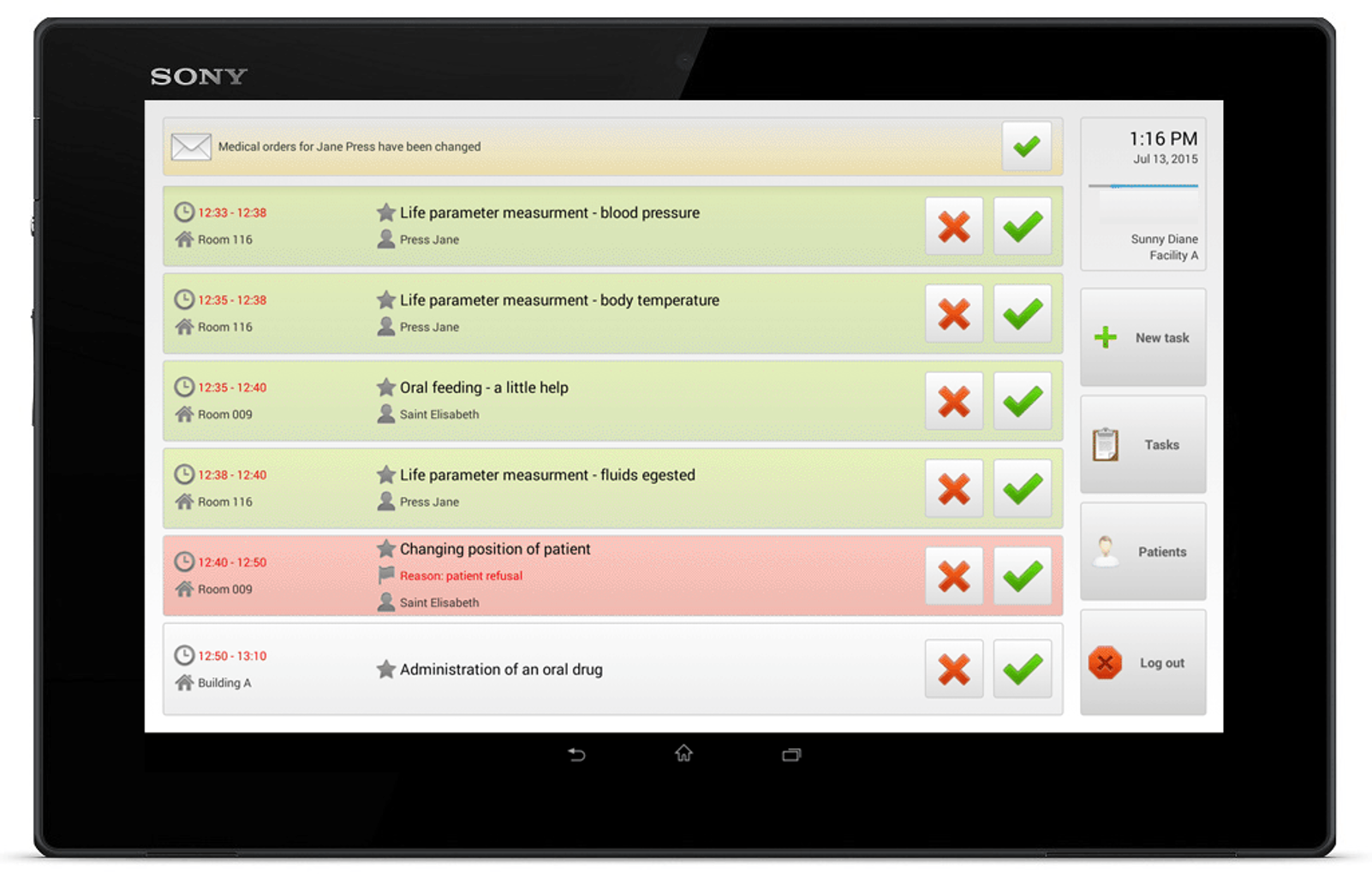
The staff member check their work plan using the mobile application available on the tablets placed in different parts of the facility. The staff member then records activity against each assigned task; in respect of medical tasks, they also provide medical results such as temperature, pressure, blood glucose levels. Follow-up protocols are automatically initiated by the system if reported medical results are out of norm. If the employee is not able to perform a task, they select a reason why the task was not performed (lack of time, performed by the family, patient refusal, etc.), and the system will notify the Care Manager about it.
Depending on the situation, the Care Manager decides whether the task needs to be performed at a later time by this or another staff member.
Each performed and assigned task is registered in the system. Collecting such detailed data provides huge analytical potential, leading to accurate diagnosis and enables organisations to make data driven decisions.
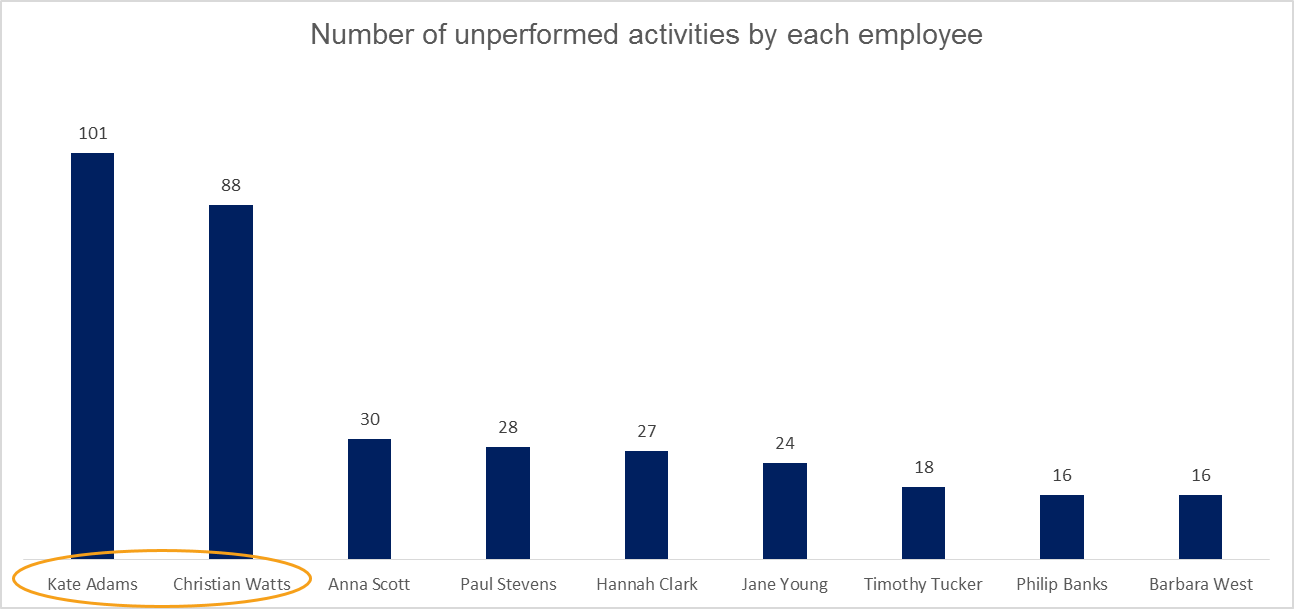
With the data collected in SupraCare, for the first time organisations can answer the questions that are essential to make patient or client care more effective: How much time does the care for each patient or client take? What is the cost of care for each patient or client? Which staff member performed most of the tasks? Which staff member performed least of the tasks? Could the scheduled tasks be performed by a smaller number of employees? Could staff perform more tasks at their duty?
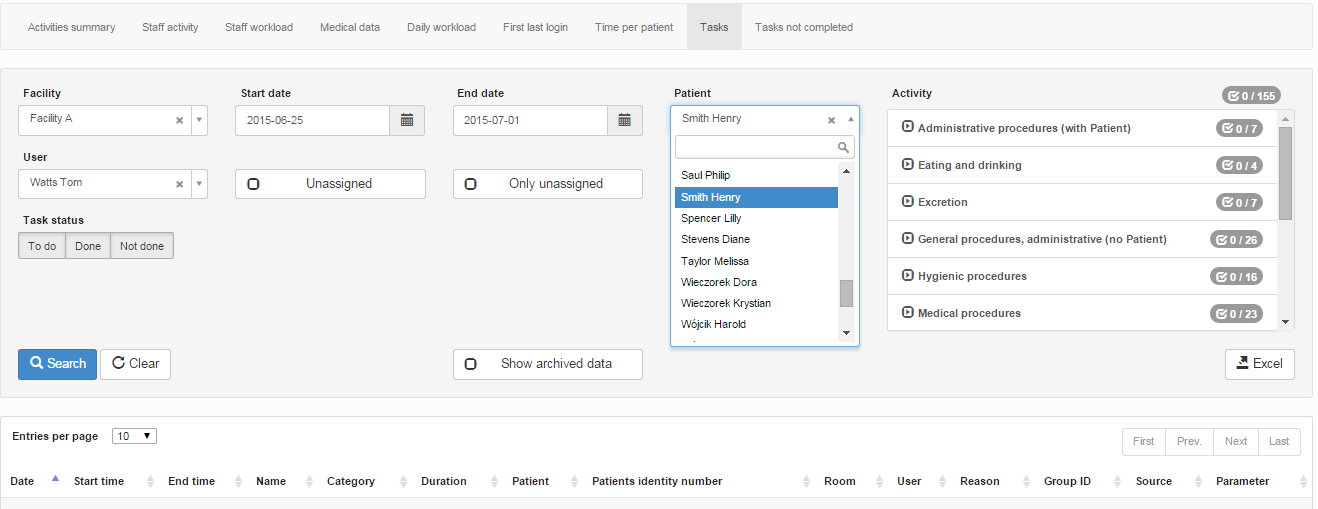
The answers to these and other questions can be found using the Reports module. All of these and related elements affect both the service quality and an organisation’s economic efficiency. Full and straightforward information is essential in order to make the necessary changes as well as to respond quickly to adverse clinical and management events.
Reports can be extracted for any period of time. For example, while looking for information about activities not performed, we can ask the following question: What activities weren’t performed? What were the reasons for not performing them? Which staff member did not perform the activities? Which patient or client refused the activity?
By asking these and other modified questions, organisations can identify any problems and determine solutions. Data driven decisions lead to higher efficiency, better quality of care and increased patient/client safety.

